
Content
Module 5: Procedure - Advanced Knowledge
Difficulty visualizing the larynx
Causes
- Reduced airspace passage due to sedation, edema or obesity
- Supraglottic mass
- Distorted anatomy or deviated larynx
- Vision obscured by blood or secretions
- "Red out" – scope is likely to be in the piriform fossa or esophagus, or impacted on mucosa
Remedies
- Ask patient to protrude the tongue or phonate or breathe deeply. Alternatively, the tongue may be retracted by an assistant holding it between a folded gauze
- Use an oral intubating device
- If an oral intubating device is already in place, ensure that it is midline and withdraw slightly
- Get assistant to perform gentle jaw thrust - this elevates the tongue and epiglottis away from the posterior pharyngeal wall and opens the path
- Suction any blood or secretions with the bronchoscope or a Yankauer sucker
- Sit patient up if currently supine
- Withdraw bronchoscope slightly and ensure that it is midline
- If necessary, withdraw bronchoscope and ensure that the tip is not covered with secretions.
Difficulty advancing the ETT over the bronchoscope
The ETT can get "caught" when passing through the vocal cords, often on the right arytenoid.
Causes
- Left facing bevel results in the tip of the ETT impinging on the right arytenoid
- Deviation of the ETT from the bronchoscope due to the gap between the two
- When performing a nasal intubation, the ETT can become impinged on the epiglottis
Remedies
- Rotate the ETT 90° anticlockwise on the bronchoscope resulting in the bevel facing 6 o'clock, minimizing impingement on the right arytenoid
- Use a larger bronchoscope or smaller ETT to reduce the size discrepancy between the two
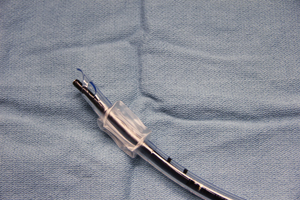
_sm.jpg)
Size 6 ETT used with adult bronchoscope results in less size discrepancy between ETT and bronchoscope.
- Use an ETT with a tapered tip (intubating LMA ETT, Parker Flex-tip® tube)
- Use a 'gap filler' between the bronchoscope and ETT (either a smaller, uncuffed ETT or the Aintree catheter)
_sm.jpg)
- Ask the patient to inhale deeply and attempt to advance the ETT gently on peak inspiration
- Rotate ETT 90° CLOCKWISE – bevel up, if the site of impingement is the epiglottis
- Use a video laryngoscope (eg: GlideScope) in addition to the Bronchoscope to assist with visualizing where the ETT is impinging
Tube-first approach vs. bronchoscope-first approach
Tube first: The ETT is inserted to the back of the nasal cavity, then the bronchoscope is passed through the ETT. The bronchoscope then acts as a 'bougie' allowing the ETT to be railroaded over it.
| ETT First | Bronchoscope First |
|
Advantages:
Disadvantages:
|
Advantages:
Disadvantages:
|
Tips
- Always keep the target structure in the center of screen.
- Use small efficient movements of the bronchoscope.
- The operator should be comfortable. Arm fatigue is common if the scope is being held too high, so either lower the bed or stand on a step to allow the scope to hang freely. Hyperextension of the knees and low back strain can be reduced by elevating one leg on a stool.
- Ask the patient to take a deep breath and synchronize advancement of the ETT with vocal cord abduction.
- A small piece of tape applied to the ETT to keep it on the scope until released will prevent it from dropping.
- Warm the ETT with warm water to soften the tube and reduce fogging (especially when using a standard ETT).
- Usual depth for nasal intubation: 26 cm for women and 28 cm for men.
Tips to prevent fogging:
- Use an anti-fog solution on the tip of the bronchoscope.
- Apply 2L/min of oxygen through the working channel of the scope.
